| Case Report |
|
|
1Department of Pathology, Princess Margaret Hospital, Hong Kong, China;
2Department of Pathology, Prince of Wales Hospital, Hong Kong, China;
3Department of Surgery, Princess Margaret Hospital, Hong Kong, China;
4Department of Pathology, Nethersole Hospital, Hong Kong, China
Corresponding Author: Tommy R. Tong, MD, AW Pathology Medical Group, 1700 “C” Street, Bakersfield, CA 93301. Tel: 661-889-8218; Fax: 661-885-5297; E-mail: tommytong@yahoo.com.
| |
ABSTRACT |
|
|
INTRODUCTION |
|
|
METHODS |
|
|
RESULTS |
|
|
DISCUSSION |
|
|
REFERENCES |
|
|
ABSTRACT
|
|---|
Pancreatic mucinous cystic neoplasms (PMCN) predominantly affect women in the reproductive age, are located in the body and tail of the pancreas, and share morphological features with similar tumors of the ovary. We report the detection of human papillomavirus (HPV) using several different PCR protocols in a borderline PMCN from a female patient. Type-specific PCR demonstrated the HPV to be type 16. If confirmed by others, this group of neoplasms might become preventable by HPV vaccination.
KEY WORDS:
pancreatic mucinous cystic neoplasm; human papillomavirus; pancreas; carcinoma
|
|
INTRODUCTION |
|---|
Pancreatic cancers are a heterogeneous group of tumors with significantly different clinical features, anatomic locations, histopathological features, molecular pathogenesis, and prognosis. The majority of these tumors are highly malignant adenocarcinomas, occur in the head of the pancreas (PANCA), and have a higher incidence in men. Pancreatic mucinous cystic neoplasms (PMCN) and solid-pseudopapillary tumor are rare tumors which occur mostly in women, the latter nearly exclusively so. Early detection and complete resection of these tumors offer a much better clinical outcome than PANCA. These differences suggest that different etiologic agents and intracellular pathways may be involved in tumorigenesis. Recently, a series of ovarian adenocarcinomas was reported in which oncogenic HPV were found. Synchronous and metachronous endocervical adenocarcinomas positive for the same HPV types were identified (1). We posit HPV as an etiologic agent in a recent case of PMCN, which histologically resembles ovarian mucinous adenocarcinomas.
|
|
CLINICAL AND PATHOLOGIC FINDINGS
|
|---|
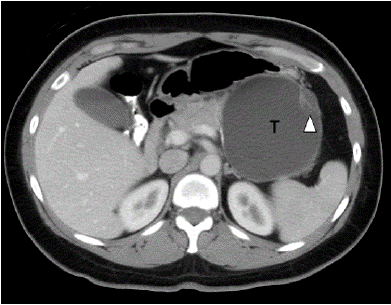
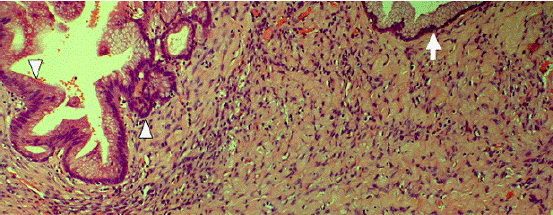
The patient is a previously healthy 45 year-old woman who experienced epigastric pain for several days before presentation. Physical examination showed a firm left upper quadrant abdominal mass. There was no tenderness or ascites. No lymphadenopathy was found. Rectal and vaginal examinations were negative for pelvic mass. Serum amylase level was normal. Abdominal ultrasonography revealed a large cystic lesion at the tail of the pancreas. Computerized axial tomography confirmed the presence of a thin walled cystic lesion with peripheral septations arising from the pancreatic tail, measuring 12 ×11 × 9 cm (Fig. 1). Distal pancreatectomy was performed. Grossly, the tumor was cystic, comprising one large locule and several smaller daughter cysts (Fig. 2). The contents were mucoid. The resection margins were not involved. Microscopically, the epithelial lining was composed of a single layer of columnar epithelial cells with foveolar architecture and focal intestinal differentiation (Fig. 3). The stroma immediately underlying the epithelial lining was focally cellular and resembled ovarian stroma. The patient recovered from the operation uneventfully. Four weeks after surgery, she consented to a Papanicolaou smear and underwent colposcopic examination of the cervix, both of which were normal. She remained disease free for at least six months.
|
|
|
| |
|---|
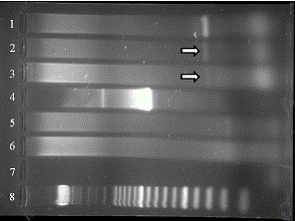
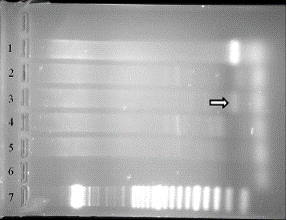
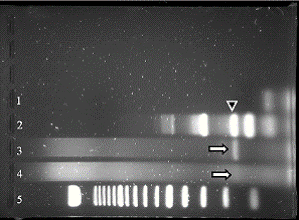
Tissue blocks with tumor and non-neoplastic pancreatic tissue were selected for HPV detection by general primer and type-specific PCR as previously reported (2-4). In brief, ten 10 μm paraffin sections were made from the paraffin blocks and DNA extracted after the standard proteinase K-phenol chloroform treatment. The purified DNA was precipitated with absolute ethanol and dissolved in 100 μl distilled water. 10 μl of the extracted DNA was used for the detection of HPV by PCR method. The general primer GP5+/6+, which amplifies a region of 140 to 150 bp in the L1 open reading frame of a broad spectrum of HPV genotypes were employed initially (5). For GP5+/6+ negative reactions, the second general primer PCR SPF1/2, which has a higher sensitivity and amplifies a 65 bp segment of the L1 region was performed (6). In addition, type-specific PCR was employed for positive specimens (7). The type-specific PCR consisted of two separate reactions, which detect HPV 6, 16 and 33, and HPV 11, 18 and 31, respectively. To assess the quality of extracted DNA, human beta-actin PCR was performed in parallel. To prevent carryover contamination, tissue blocks were cut with new blades after prior decontamination of the microtome and instruments. DNA extraction and purification, master-mix set-up, PCR amplification, as well as post-amplification gel electrophoresis were all carried out in dedicated areas. Uni-directional workflow for the PCR processes was followed. All pipetting works were conducted with the use of disposable aerosol-resistant micropipette tips.
HPV was identified in tumor blocks by general primer PCR reactions employing GP5+/6+ (Fig. 4) and SPF1/2 primers (Fig. 5). Type-specific PCR identified the HPV as type 16, a member of the high-risk HPVs (Fig. 6). Non-neoplastic pancreatic tissue and water negative controls were consistently negative for HPV. General primer PCR employing primer pairs MY09/11 was negative (Fig. 4).
|
|
|
|
|
DISCUSSION |
|---|
Pancreatic mucinous cystic neoplasms are of unknown etiology and are much more common in women than in men. Its location in the body and tail of the pancreas is in contrast to conventional pancreatic adenocarcinoma of the head of the pancreas (PANCA), which has a higher incidence in men (8). The evolution of PMCN is slow, giving a larger window for curative resection. Malignant progression takes place in the epithelial component but can also occur in the mesenchymal component, giving rise to sarcomas such as malignant fibrous histiocytoma. Fully malignant tumors are associated with oncogenic K-ras mutations and over-expression of EGFR and inactivation of tumor suppressors p53 and DPC4.
In terms of molecular pathways involved, PMCN differs from PANCA in being mostly negative for immunohistochemical expression of p53 (10). In uterine cervical carcinomas, which almost exclusively contain oncogenic HPV, high-risk HPV E6 targets p53 for proteasomal degradation, keeping p53 at a low level. As expected, most pre-malignant cervical lesions and a significant fraction of invasive cervical carcinomas are negative for p53 over-expression (11). This lends support to a possible etiologic link between HPV and PMCN. However, it is also possible that the p53 pathway may be alternatively disrupted, for example by over-expression of hDM2.
Recently, a series of ten ovarian adenocarcinomas was reported, having synchronous and metachronous HPV-induced endocervical adenocarcinomas, some masquerading as pre-invasive lesions (1). Pancreatic cancers, including an example of PMCN have occurred synchronously or metachronously with ovarian mucinous adenocarcinomas (12). There was no mention of endocervical adenocarcinoma in the report, which attributes the ovarian cancers to metastasis from the pancreatic cancers. In another report, PMCN occurred synchronously with ovarian mucinous cystadenoma, thought to represent independent primaries (13). Thus, ovarian carcinomas have occurred synchronously with endocervical adenocarcinoma and with PMCN.
The hypothesis of PMCN being caused by HPV is novel, as we were not able to find similar case report in the English language medical literature. How the pancreas is infected by HPV is unknown. It is more likely to be the seat of metastasis from an occult primary elsewhere that is caused by HPV. A search for occult tumors, for example in the endocervix, and testing for HPV in PMCN will help to confirm or refute an etiologic link of oncogenic HPV and PMCN. On June 8, 2006, the U.S. Food and Drug Administration licenses the recombinant HPV vaccine GardasilÒ as a vaccine for the prevention of cervical cancer and other diseases in females caused by HPV. The vaccine was developed against HPV types 6, 11, 16 and 18. Clinical trials have demonstrated near 100% efficacy in protection against precancerous lesions caused by types 16 and 18, which are oncogenic. If PMCN is indeed caused by high-risk HPVs, vaccination against these epitheliotropic viruses might also prevent these tumors.
In summary, employing different PCR protocols, we consistently detected human papillomavirus, typed as the oncogenic HPV16, in a pancreatic mucinous cystic neoplasm. Further studies of these tumors are warranted.
|
|
REFERENCES
|
|---|
1. Elishaev E, Gilks CB, Miller D, Srodon M, et al. Synchronous and metachronous endocervical and ovarian neoplasms: evidence supporting interpretation of the ovarian neoplasms as metastatic endocervical adenocarcinomas simulating primary ovarian surface epithelial neoplasms. Am J Surg Pathol 2005; 29(3):281.
2. Chan MK, Lau KM, Tsui Y, Wong FW, et al. Human papillomavirus infection in Hong Kong Chinese women with normal and abnormal cervix--detection by polymerase chain reaction method on cervical scrapes. Gynecol Oncol 1996; 60(2):217.
3. Lee CN, Cavanagh HM, Lo ST, Ng CS. Human papillomavirus infection in non-neoplastic uterine cervical disease in Hong Kong. Br J Biomed Sci 2001; 58(2):85.
4. Qu W, Jiang G, Cruz Y, Chang CJ, et al. PCR detection of human papillomavirus: comparison between MY09/MY11 and GP5+/GP6+ primer systems. J Clin Microbiol 1997; 35(6):1304.
5. Jacobs MV, Snijders PJ, van den Brule AJ, Helmerhorst TJ, et al. A general primer GP5+/GP6 (+)-mediated PCR-enzyme immunoassay method for rapid detection of 14 high-risk and 6 low-risk human papillomavirus genotypes in cervical scrapings. J Clin Microbiol 1997; 35(3):791.
6. Kleter B, van Doorn LJ, ter Schegget J, Schrauwen L, et al. Novel short-fragment PCR assay for highly sensitive broad-spectrum detection of anogenital human papillomaviruses. Am J Pathol 1998; 153(6):1731.
7. van den Brule AJ, Meijer CJ, Bakels V, Kenemans P, et al. Rapid detection of human papillomavirus in cervical scrapes by combined general primer-mediated and type-specific polymerase chain reaction. J Clin Microbiol 1990; 28(12):2739.
8. Thompson LD, Becker RC, Przygodzki RM, Adair CF, et al. Mucinous cystic neoplasm (mucinous cystadenocarcinoma of low-grade malignant potential) of the pancreas: a clinicopathologic study of 130 cases. Am J Surg Pathol 1999; 23(1):1.
9. Wouters K, Ectors N, Van Steenbergen W, Aerts R, et al. A pancreatic mucinous cystadenoma in a man with mesenchymal stroma, expressing oestrogen and progesterone receptors. Virchows Arch 1998; 432(2):187.
10. Zhang SY, Ruggeri B, Agarwal P, Sorling AF, et al. Immunohistochemical analysis of p53 expression in human pancreatic carcinomas. Arch Pathol Lab Med 1994; 118(2):150.
11. Tervahauta AI, Syrjanen SM, Vayrynen M, Saastamoinen J, et al. Expression of p53 protein related to the presence of human papillomavirus (HPV) DNA in genital carcinomas and precancer lesions. Anticancer Res 1993; 13(4):1107.
12. Young RH, Hart WR. Metastases from carcinomas of the pancreas simulating primary mucinous tumors of the ovary. A report of seven cases. Am J Surg Pathol 1989; 13(9):748.
13. Gagne LJ, Colacchio T, Longnecker DS. Simultaneous mucinous cystadenoma of ovary and mucinous cystadenocarcinoma of pancreas. Int J Pancreatol 2000; 28(1):9.